Pigs, birds, and humans are each susceptible to many flu viruses. Typically, these viruses infect only one species. However, sometimes these viruses swap genes and create new viruses that can infect more than one species. Even then, new viruses that are capable of infecting two species typically are very difficult to transmit from human to human. Sometimes, however, further recombinations or mutations of genes create a virus that can spread rapidly among humans – thus creating a global pandemic. The worst global pandemic in modern times was the flu pandemic of 1918-1919. It affected about a third of the human race and killed at least 40 million people in roughly 1 year.

Simultaneous Appearance in Humans and Swine (1918)
Before 1918, influenza in humans was well known, but the disease had never been described in pigs. For pig farmers in Iowa, everything changed after the Cedar Rapids Swine Show, which was held in September of that year. Just as the 1918 pandemic spread the human influenza A (H1N1) virus worldwide and killed 40 million to 50 million people, herds of swine were hit with a respiratory illness that closely resembled the clinical syndrome affecting humans. Similarities in the clinical presentations and pathologic features of influenza in humans and swine suggested that pandemic human influenza in 1918 was actually adapted to the pig, and the search for the causative agent began.
The breakthrough came in 1931 when Robert Shope, a veterinarian, transmitted the infectious agent of swine influenza from sick pigs, by filtering their virus containing secretions, to healthy animals.
CNN March 2009
Doctors: No definitive answers on flu deaths among young
For most, the flu is a winter inconvenience -- stuffy nose, fever, body aches and a few days of bed rest. But what seems fairly routine also can become life-threatening. The virus causes inflammation throughout the body and disturbs the functions of the body, including breathing. Typically half of the flu deaths occur in children who have degenerative heart or lung disease or immune risk factors, but the other half are seemingly healthy.
"There isn't a good understanding of why that happens," said Dr. John Treanor, professor of medicine and of microbiology and immunology at the University of Rochester School of Medicine.
"There's speculation that these children, for genetic reasons, had unusual immune response to the flu, resulting in deaths."
August 26, 2009
CDC Confirms Ties to Virus First Discovered in U.S. Pig Factories
Starting in the early 1990s, the U.S. pig industry restructured itself after Tyson's profitable chicken model of massive industrial-sized units. As a headline in the trade journal National Hog Farmer announced, "Overcrowding Pigs Pays—If It's Managed Properly."
The majority of U.S. pig farms now confine more than 5,000 animals each.
Researchers also found that when farms were packed close together, as is increasingly the case in high pig-density areas of North America and Europe, pigs appeared to have up to 16.7 times the odds of testing positive for swine flu. "Close location enhances the possibility for windborne, personnel, and fomites disease transmission from one farm to another." The "spread of pig slurry [urine and feces]" on nearby land may also play a role.
JealousBrother.com
August 10th, 2009
What does the CDC consider a confirmed case of Swine Flu?
The CDC uses the following guidelines: A confirmed case of novel influenza A (H1 N1 ) virus infection is defined as a person with an
Influenza-like illness (ILI is defined as fever (temperature of 100°F [37.8°C] or greater) and a cough and/or a sore throat in the absence of a KNOWN cause other than influenza.) with laboratory confirmed novel influenza A (H1 N1 ) virus infection by one or more of the following tests:
1. real-time RT-PCR
2. viral culture
The CDC has this to say about the real-time RT-PCR test, “If reactivty of real-time RT-PCR for influenza A is strong it is more suggestive of a novel influenza A (H1 N1 ) virus. Confirmation as novel influenza A (H1 N1 ) virus by real-time RT-PCR was originally performed only at CDC, but at this time may be available in your state public health laboratory ."
The CDC has this to say about Viral Cultures: “Isolation of novel influenza A (H1 N1 ) virus is diagnostic of infection, but may not yield timely results for clinical management. A negative viral culture does not exclude infection with novel influenza A (H1 N1 ) virus.”
So what exactly am I getting at? There is no way for a physician or health organization to definitively tell a patient whether they have H1 N1 , H3 N2 , or any other Influenza A sub-type (Which includes seasonal flu) when using readily available RIDT’s. The only diagnostic results come from the lengthy process of laboratory analyzed cultures and rRt-PCR swine flu panels.
2008 Oct
Influenza vaccine effectiveness among children 6 to 59 months of age during 2 influenza seasons
Strong Memorial Hospital, Rochester, NY
OBJECTIVE: To measure vaccine effectiveness (VE) in preventing influenza-related health care
visits among children aged 6 to 59 months during 2 consecutive influenza seasons.
CONCLUSION: In 2 seasons with suboptimal antigenic match between vaccines and circulating
strains, we could not demonstrate VE in preventing influenzarelated
inpatient/ED or outpatient visits in children younger than
5 years.
“Surprisingly little information exists regarding influenza vaccine effectiveness among young children receiving vaccine in routine health care settings.”
Oct. 21, 2009
Swine Flu Cases Overestimated?
Study Of State Results Finds H1N1 Not As Prevalent As Feared
If you've been diagnosed "probable" or "presumed" 2009 H1N1 or "swine flu" in recent months, you may be surprised to know this: odds are you didn’t have H1N1 flu. In fact, you probably didn’t have flu at all. That's according to state-by-state test results obtained in a three-month-long CBS News investigation.
The ramifications of this finding are important. According to the Centers for Disease Control and Prevention (CDC) and Britain's National Health Service, once you have H1N1 flu, you're immune from future outbreaks of the same virus. Those who think they've had H1N1 flu -- but haven't -- might mistakenly presume they're immune. As a result, they might skip taking a vaccine that could help them, and expose themselves to others with H1N1 flu under the mistaken belief they won't catch it. Parents might not keep sick children home from school, mistakenly believing they've already had H1N1 flu.
NOVEMBER 2009 ATLANTIC
Does the Vaccine Matter?
More than 200 known viruses and other pathogens can cause the suite of symptoms known as “influenza-like illness”; respiratory syncytial virus, bocavirus, coronavirus, and rhinovirus are just a few of the bugs that can make a person feel rotten. And depending on the season, in up to two-thirds of the cases of flu-like illness, no cause at all can be found.
. The only way to know if someone has the flu—as opposed to influenza-like illness—is by putting a Q-tip into the patient’s throat or nose and running a test, which simply isn’t done that often. Likewise, nobody really has a handle on how many of the deaths that are blamed on flu were actually caused by a flu virus, because few are confirmed by a laboratory. “I used to be a family physician,” says Jefferson. “I’ve never seen a patient come to my office with H1N1 written on his forehead. When an old person dies of respiratory failure after an influenza-like illness, they nearly always get coded as influenza.”
“Launched early enough and continued long enough, social distancing can blunt the impact of a pandemic,” says Howard Markel, a pediatrician and historian of medicine at the University of Michigan.
Washing hands diligently, avoiding public places during an outbreak,
and having a supply of canned goods and water on hand are sound
defenses, he says. Such steps could be highly effective in helping to slow the spread of the virus.
Fear of Flu: Shifting the Goalposts
KAISER HEALTH NEWS
NOV 2009
Is the 2009 H1N1 more dangerous than garden variety seasonal flu, for healthy kids compared to kids with underlying illnesses? According to a paper published last month in the New England Journal of Medicine, probably not. The authors found that 60 percent of children who were hospitalized with swine flu had underlying illnesses. In years past, only 31 to 43 percent of children who were hospitalized with seasonal flu had similar underlying illnesses – meaning that the rate at which 2009 H1N1 causes serious illness in healthy children is lower than with seasonal flu.
As of August 31, however, the CDC said that anyone 18 years or older who dies with a syndrome known as influenza-like illness, or ILI, can be included in the count. The CDC has no requirement for uniform reporting of flu deaths by the states. Twenty-eight states, according to the agency, report only laboratory-confirmed flu deaths, while the others are now reporting deaths that look to doctors like they might be the result of flu.
That decision could dramatically inflate the numbers of reported flu deaths this year. By the CDC's weekly estimate, when doctors think a patient has the flu, they are wrong between 46 and 82 percent of the time.
Why should any of this matter? In part, because statistics, when filtered by the popular media, can scare the daylights out of the public and feed pandemic worries that may not be justified. The numbers also matter to public policy. As reported deaths rise, the CDC tends to enlarge its recommendation for who should be vaccinated, and who should receive anti-viral drugs. For example, based on rising pediatric deaths, the CDC issued new recommendations in 2009 that all children from 6 months to 18 years should get the flu vaccine each year. Previously, the vaccine was recommended only for high-risk children.
Pandemic preparedness for swine flu influenza in the United States.
In March and early April 2009, Mexico experienced outbreaks of influenza caused by the H1N1
virus, which has spread throughout the world. With the pandemic of H1N1 infections, we have
discussed in this scientific article strategies that should limit the spread of the influenza A (H1N1)
virus in our country. Specific vaccines against the influenza H1N1 virus are being manufactured,
and a licensed vaccine is expected to be available in the United States by mid-October 2009.
However, some health-care workers may be hesitant to take a vaccine because it contains a
mercury preservative-thimerosal-which can be harmful to their health. When caring for patients
with respiratory infections, the health-care worker should be wearing a facial respirator. In a report
from the Centers for Disease Control and Prevention (CDC), it was indicated that each healthcare
professional should be required to do a respiratory fit testing to identify the ideal model.
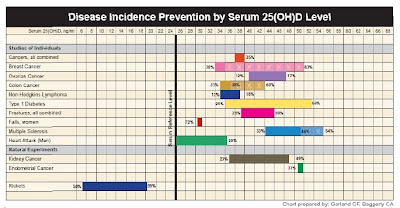
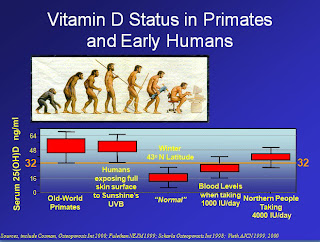
Because it has been well documented that a vitamin D deficiency can
precipitate the influenza virus, we strongly recommend that all health-care
workers and patients be tested and treated for vitamin D deficiency to
prevent exacerbation of a respiratory infection.
11/20/2009
By Sen. Joseph Lieberman
Homeland Security and Governmental Affairs Committee Chairman
While this new flu strain is affecting most people mildly, it has affected a small percentage
severely, and vaccine production problems have meant that some identified by the Department of
Health and Human Services as high risks for infection have not been able to get inoculated.
HHS promises national delivery of millions vaccine doses a week for the next few months.
But it does not ease my own concerns about HHS' miscalculations….Furthermore, unlike traditional seasonal flu that disproportionally affects the elderly, the H1N1 virus is impacting young people, with over 50 percent of hospitalizations and a quarter of all deaths occurring in people under the age of 25. Alarmingly, young children are at very serious risk, with about 540 pediatric deaths tallied so far.
I LIKE JOE LIEBERMAN, BUT SENATORS SHOULD USE ACCURATE NUMBERS WHICH ARE MORE AVAILABLE TO THEM THAN ANY CITIZEN IN ORDER NOT TO FRIGHTEN THEIR CONSTITUENTS. THE NUMBERS FROM THE CDC ON NOV 21, 2009 RECORD 243 PEDIATRIC DEATHS.
WHO’S TELLING THE TRUTH? – A BIG PROBLEM DURING THE SWINE PANIC
December 10, 2009, 1:00 p.m.
THOMAS FRIEDEN, DIRECTOR OF THE CDC
Thomas Frieden: Good afternoon, everybody. Today we're releasing new estimates as we said we would. The bottom line is that by November 14th, the day up to which those estimates include, many times more children and younger adults, unfortunately, have been hospitalized or killed by H1N1 influenza than occurs during a regular flu season.
What we have seen so far reiterates that people under the age of 65 are most heavily impacted by influenza. By November 14th, many times more children and younger adults, unfortunately, have been hospitalized or killed by H1N1 influenza than happens in a usual flu season. Specifically, there have been, we estimate there have been nearly 50 million cases, mostly in younger adults and children. More than 200,000 hospitalizations which is about the same number that there is in a usual flu season for the entire year. And, sadly, nearly 10,000 deaths, including 1,100 among children and 7,500 among younger adults. That.s much higher than in a usual flu season.,,, The estimate we have – the estimate that we're releasing here is not done in the same way that gives us the 36,000 estimate. That estimate is a different methodology. And will give a slightly larger number than this number would give. But if you were to compare, even though it's not a directly applicable comparison, under 50 in that estimate, there are less than 1,000 deaths a year in age under 50. We didn't break out in this —we’re not able to at this time, the 50 to 64 versus 50. But a large portion of those adults are under 50. So it is really many times more severe in terms of severe illness and hospitalizations are several times higher for children and young adults as well in H1N1 than in a usual flu season.
REALLY?????
THE CDC DIRECTOR’S FIGURE DOESN’T QUITE JIVE WITH THE CDC REPORT OF MARCH 2010 WHICH RECORDS 331 PEDIATRIC DEATHS.
Science
December 2009:
VIRUS OF THE YEAR: The Novel H1N1 Influenza
For years, scientists have been warning about the potential for an influenza pandemic on the order of the 1918 Spanish flu. They imagined the culprit would surface in Asia--and, since 2003, have worried that the avian influenza strain H5N1 might be it. Health officials worldwide drafted one preparedness plan after another. But the pandemic that erupted last spring looks nothing like the one in the plans. Not only did it begin in North America, but the swine virus behind it is a novel form of an H1N1 strain already circulating in humans. And although the new H1N1 is unusually dangerous for the young and for pregnant women, in most otherwise healthy people it causes a disease no more severe than seasonal flu. Scientists have repeatedly warned that this relatively mild virus could mutate or swap genes with cousins and become deadlier. But for now, it looks as if this H1N1 will go down in history more for causing confusion than catastrophe.
THE CDC HAS CONTINUED TO PUT OUT PERIODIC ESTIMATES OF PEDIATRIC DEATHS WHICH ARE EXAGGERATED BY 2-3 TIMES. THEY CONTINUE TO HAVE ADDS ON TV RECOMMENDING VACCINATION AGAINST THE H1N1 FLU EVEN THOUGH THE H1N1 HAS ESSENTIALLY LEFT THE U.S. THE LAST ARTICLE ON THE PANIC SWINE 09 BLOG IS ABOUT THE SUSPICIAN THAT MUCH ABOUT THE SWINE FLU PANDEMIC MAY HAVE BEEN DRIVEN BY MONEY!

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}